Avanzamento bimaxillare, con miglioramento estetico e funzionale
Traduzione automatica
L'articolo originale è scritto in lingua ES (link per leggerlo) .
Il trattamento delle deformità dentofacciali è evoluto in modo significativo negli ultimi dieci anni. La conoscenza dei contributi vascolari nelle osteotomie –sviluppata da William Bell–, la versatilità delle osteotomie di mascella, mandibola e mento per provocare spostamenti nelle tre dimensioni dello spazio e l'uso della fissazione rigida permettono di eseguire osteotomie precedentemente considerate instabili, come la rotazione antioraria e/o i grandi avanzamenti mascellari-mandibolari.
I progressi nella pianificazione digitale e il miglioramento delle tecniche anestetiche consentono che la chirurgia ortognatica si sia sviluppata e semplificata in modo significativo.
L'obiettivo non è più solo ottenere un'occlusione adeguata e stabile. Le nostre conoscenze e lo sviluppo di queste procedure ci permettono di ottenere un miglioramento dentale e occlusale, che sia stabile e con minime ripercussioni parodontali e/o articolari, ma anche un importante miglioramento respiratorio e obiettivi estetici difficilmente raggiungibili con altre tecniche chirurgiche. La prevedibilità della chirurgia ortognatica è superiore a qualsiasi tecnica di ricostruzione facciale, così come la sua durabilità.
I casi di classe II per ipoplasia mandibolare che solitamente venivano trattati con due estrazioni superiori hanno beneficiato di questi progressi nella chirurgia ortognatica. Così, ai nostri pazienti vengono offerti risultati molto più soddisfacenti.
Caso clinico

Un paziente di 20 anni si presenta per una valutazione e trattamento ortodontico. Il suo motivo di consulto è un “leggero affollamento negli incisivi superiori”. Dopo aver studiato il caso, vediamo che siamo di fronte a una classe II scheletrica per ipoplasia mandibolare, molto compensata dentoalveolarmente con la protrusione degli incisivi inferiori.
Questo tipo di casi, in un paziente senza crescita, eravamo soliti trattarlo con quattro estrazioni per compensare la classe II e la protrusione degli incisivi inferiori.
Questo piano di trattamento ortodontico peggiorerebbe la relazione labbro-dente, aumentando il sorriso gengivale e, naturalmente, non migliorerebbe la proiezione del terzo inferiore, mantenendo una mandibola retrusa.
I progressi nella chirurgia ortognatica attuale fanno sì che la compensazione ortodontica della classe II non sia più la nostra prima opzione di trattamento e affrontiamo casi come questo da un punto di vista combinato di ortodonzia e chirurgia ortognatica.
Analisi facciale

Nell'analisi facciale (fig. 2) abbiamo rilevato un leggero eccesso verticale mascellare, incompetenza labiale e gap aumentato, con esposizione eccessiva degli incisivi a riposo e eversione del labbro inferiore.
In posizione di sorriso, il paziente presenta una relazione labbro-dente aumentata. Il piano mascellare è livellato e c'è asimmetria nei margini gengivali.
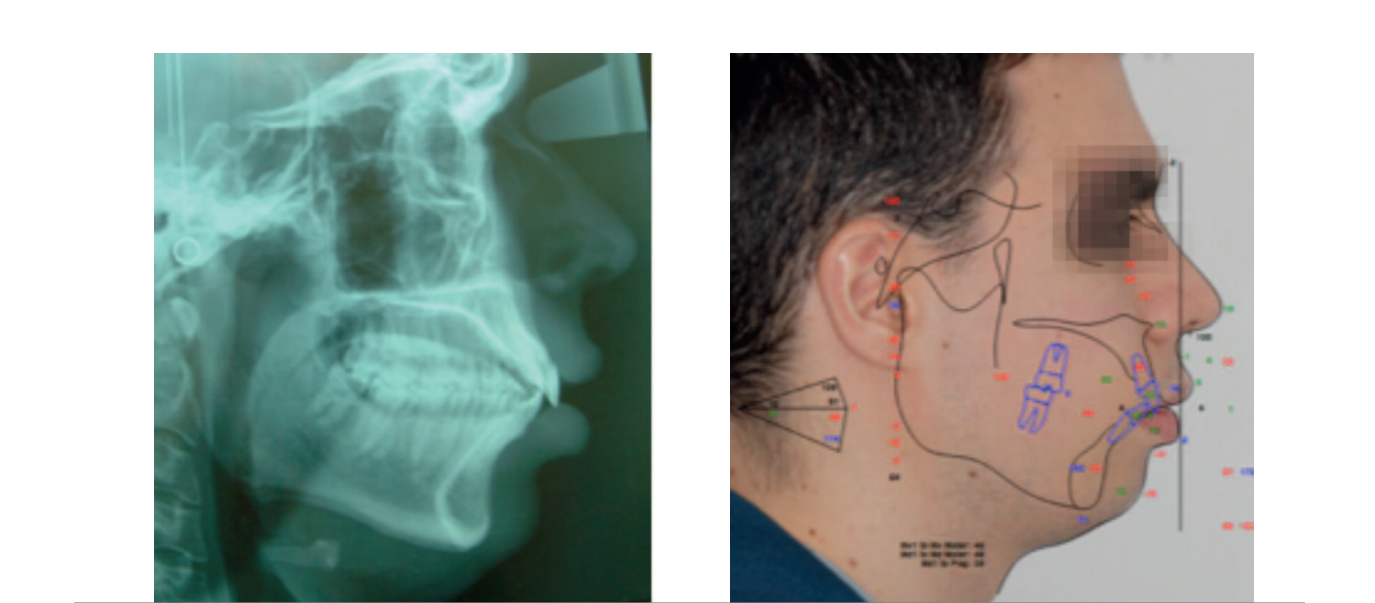
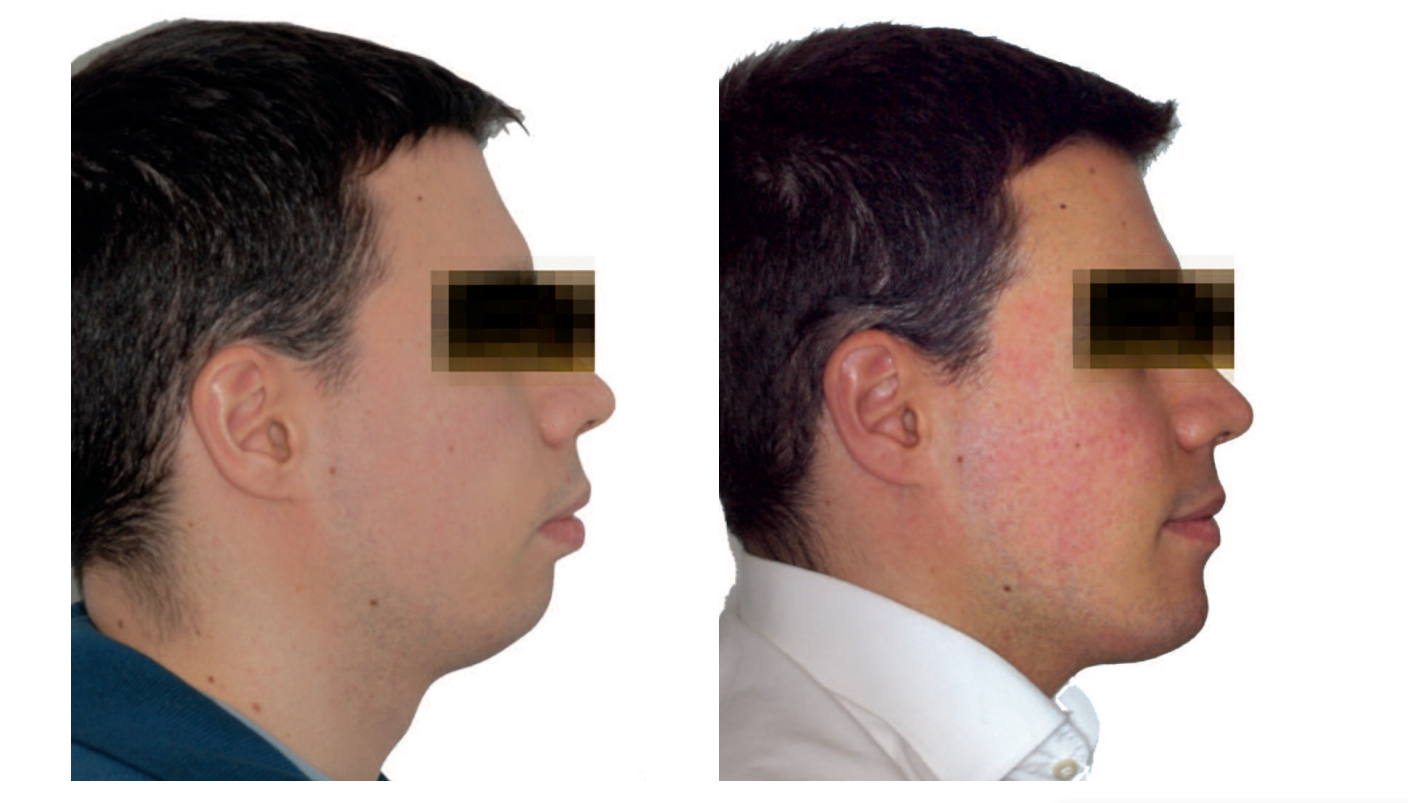
Nello studio del profilo (fig. 3) si osserva la mancanza di supporto del terzo inferiore. È un profilo di micrognazia con eversione del labbro inferiore, distanza cervicomandibolare diminuita e angolo cervicomandibolare mal definito, con flaccidità e doppio mento.

Analisi dentale
Nell'analisi dentale (fig. 4) si osserva: leggera compressione posteriore per mancanza di torsione nei molari e nei premolari; classe II molare e canina bilaterale; assenza di risalto per proinclinazione degli incisivi inferiori; affollamento anteriore in entrambe le arcate e rotazioni multiple, così come severa proinclinazione degli incisivi inferiori.


Piano ortodontico
Il piano di ortodonzia include i seguenti passaggi:
- Necessità di estrazioni dei premolari inferiori per poter retroinclinare gli incisivi inferiori.
- Gli incisivi superiori sono leggermente proinclinati. Recupereremo la loro posizione e risolveremo l'affollamento anteriore con stripping da canino a canino.
- Livellamento della curva di Spee, intrudendo gli incisivi inferiori.
- Correzione della curva di Wilson, con torsione coronovestibolare nei premolari e molari superiori.
Pianificazione chirurgica iniziale
Abbiamo deciso di avanzare il mascellare di 4 mm per ottenere una migliore protezione anteroposteriore dello stesso e, allo stesso tempo, poter avanzare la mandibola alla massima magnitudine. Il mascellare impatterà verticalmente nella sua parte anteriore e scenderà posteriormente, provocando la rotazione antioraria del piano occlusale.
Situazione prechirurgica
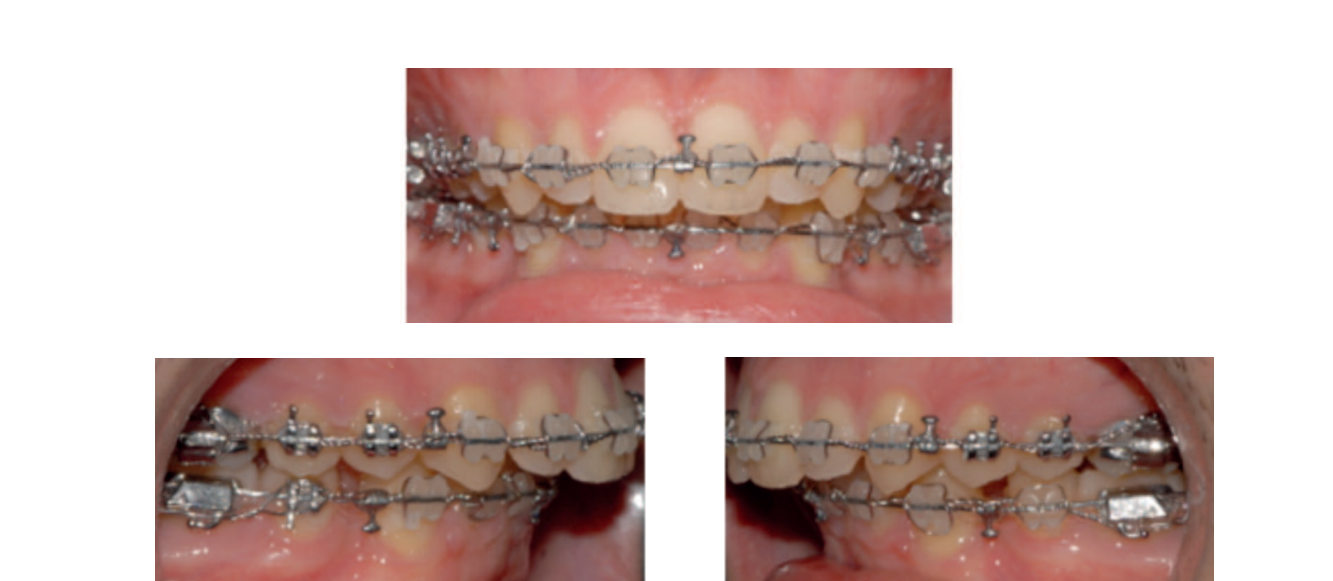

Una volta livellata la curva di Spee inferiore e corretta l'inclinazione degli incisivi inferiori, il nostro obiettivo prechirurgico ortodontico è raggiunto. La perdita di ancoraggio posteriore per chiudere gli spazi di estrazione può essere rimandata alla fase postchirurgica, approfittando del RAP (fenomeno di accelerazione regionale).
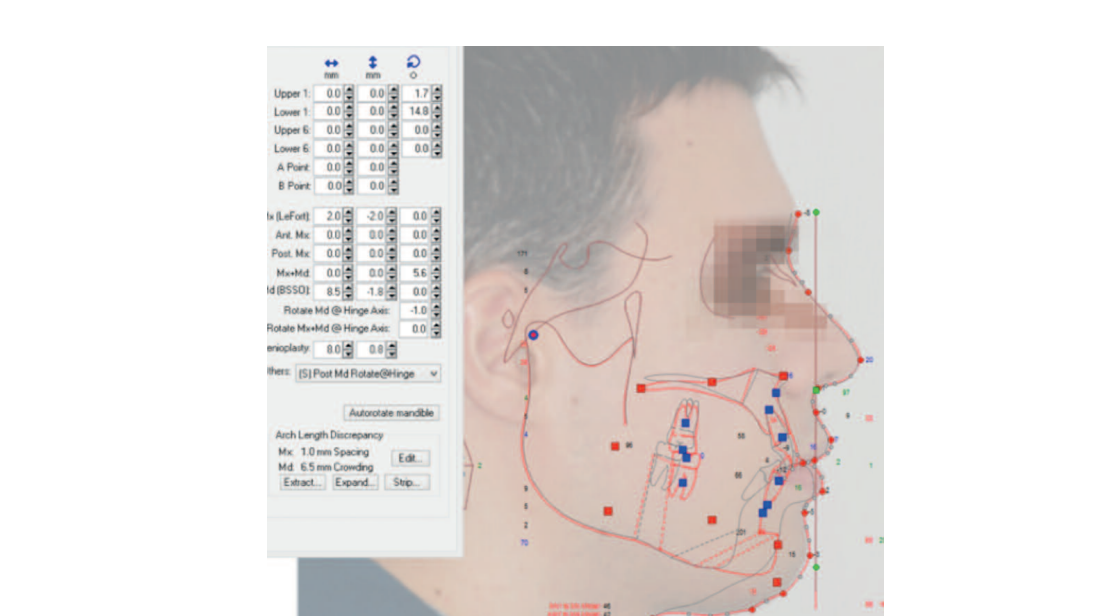
Pianificazione della chirurgia bimaxillare
Il mascellare sarà spostato in avanti di 4 mm per garantire un avanzamento mandibolare sufficiente per una proiezione mandibolare estetica. La posizione verticale finale degli incisivi superiori sarà determinata al termine della chirurgia, con i mascellari in occlusione e misurando da un punto fisso, che viene stabilito con una vite autofilettante dall'inizio della chirurgia nel nasion.
La determinazione finale della posizione degli incisivi superiori, orizzontalmente e verticalmente, influisce in modo significativo sull'estetica del sorriso. La mandibola avanzerà e sarà eseguita una mentoplastica di avanzamento e aumento verticale.
Chirurgia bimaxillare
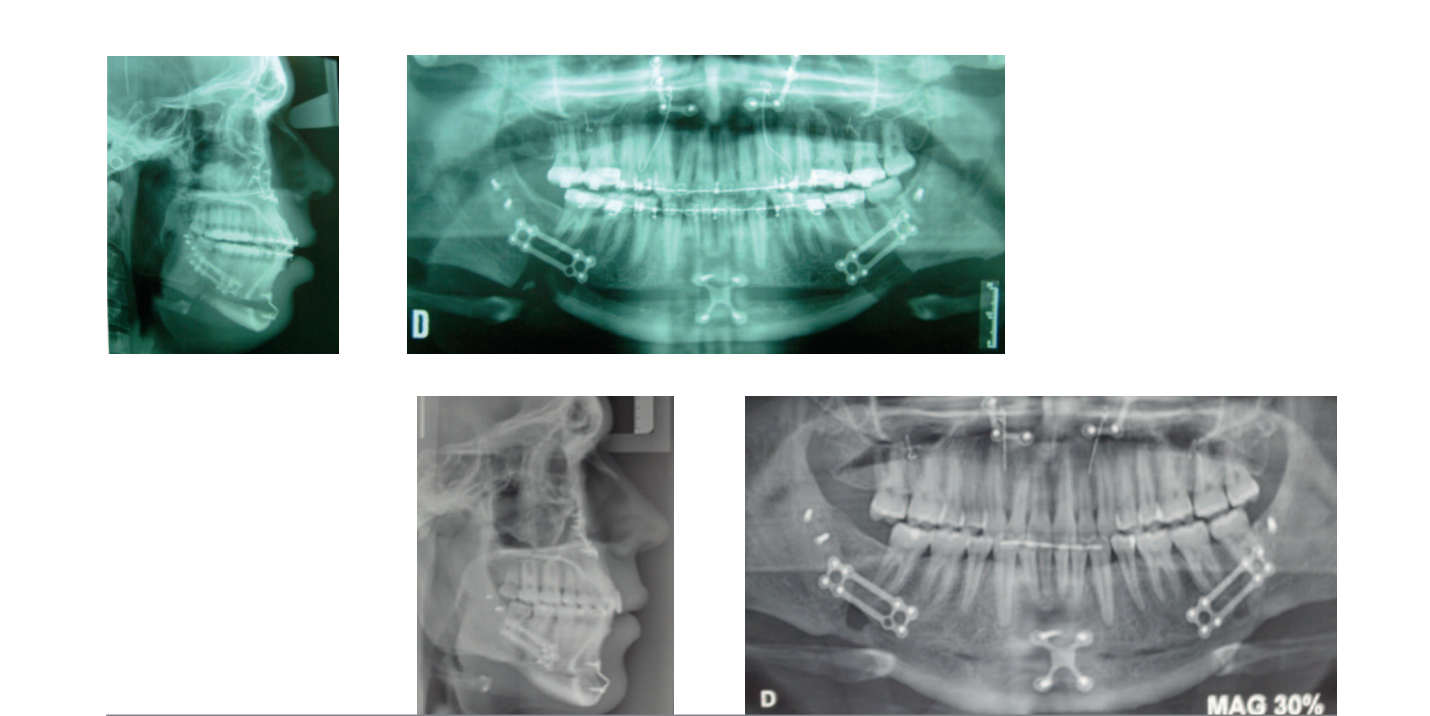
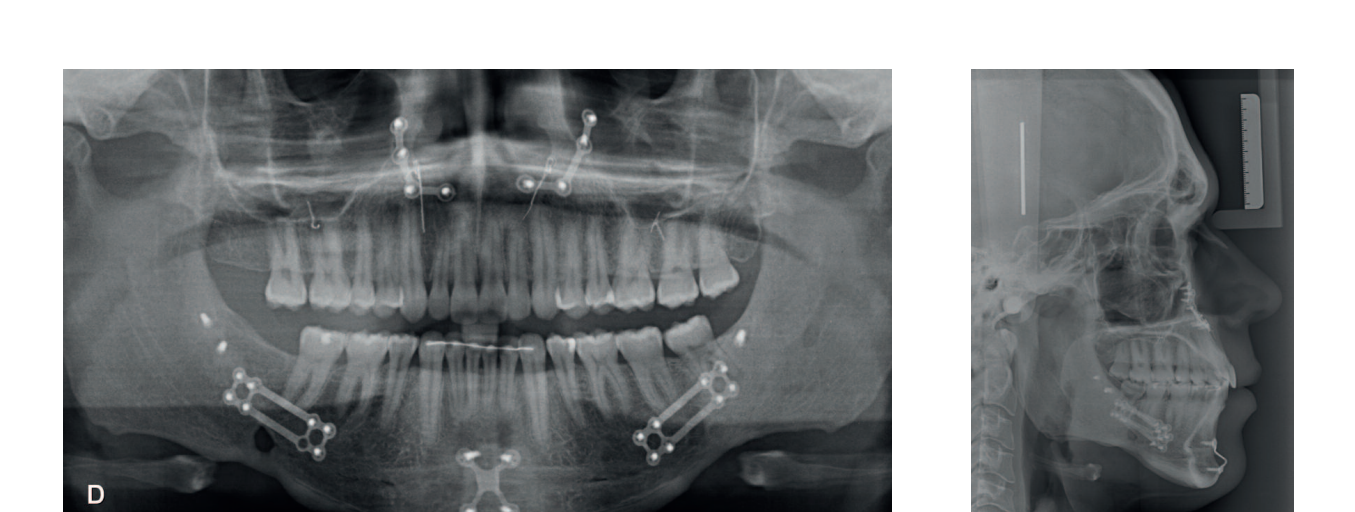
Sotto anestesia generale, è stata effettuata intubazione nasotracheale. L'intervento è iniziato con il mascellare superiore, eseguendo osteotomia Lefort I con impattamento anteriore di 2 mm, discesa posteriore di 2 mm e avanzamento di 4 mm. È stata effettuata septoplastica e resezione sottomucosa dei turbinati.
Le osteotomie sono state fissate rigidamente con due placche in arbotante piriforme e mediante fili nei zigomatici. È stata utilizzata trazione scheletrica nel mascellare posteriore.
La mandibola è stata osteotomizzata con la tecnica di Obwegeser Epker e avanzata di 14 mm. È stata effettuata una notevole separazione dei muscoli del ramo e del corpo per facilitare l'avanzamento. Le osteotomie sono state fissate in modo consistente con placche rigide di 2 mm con ponte di avanzamento. Il paziente è rimasto in terapia intensiva per 24 ore. Non è stato effettuato cerchiaggio intermascellare, sono stati posizionati elastici di classe II. È stata eseguita mentoplastica di avanzamento di 3 mm e discesa di 6 mm.
Finalizzazione e ritenzione



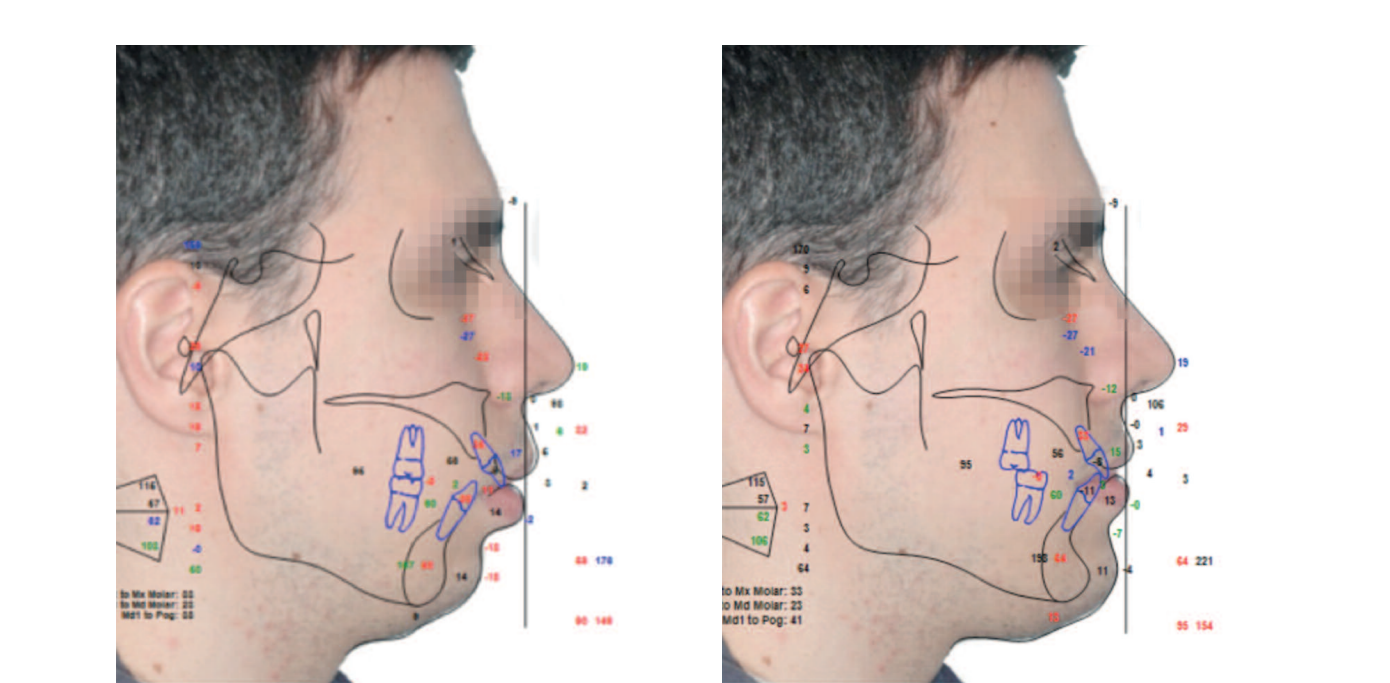
Stabilità a tre anni dal trattamento




Risultati
Il paziente evolve in modo soddisfacente e l'occlusione ottenuta è stabile. I risultati facciali dimostrano un chiarissimo miglioramento estetico.
La espansione scheletrica provocata dall'avanzamento dei mascellari con rotazione antioraria e mentoplastica comporta un miglioramento estetico ineguagliabile rispetto a qualsiasi altro tipo di chirurgia facciale. I cambiamenti a lungo termine sono stabili e duraturi.
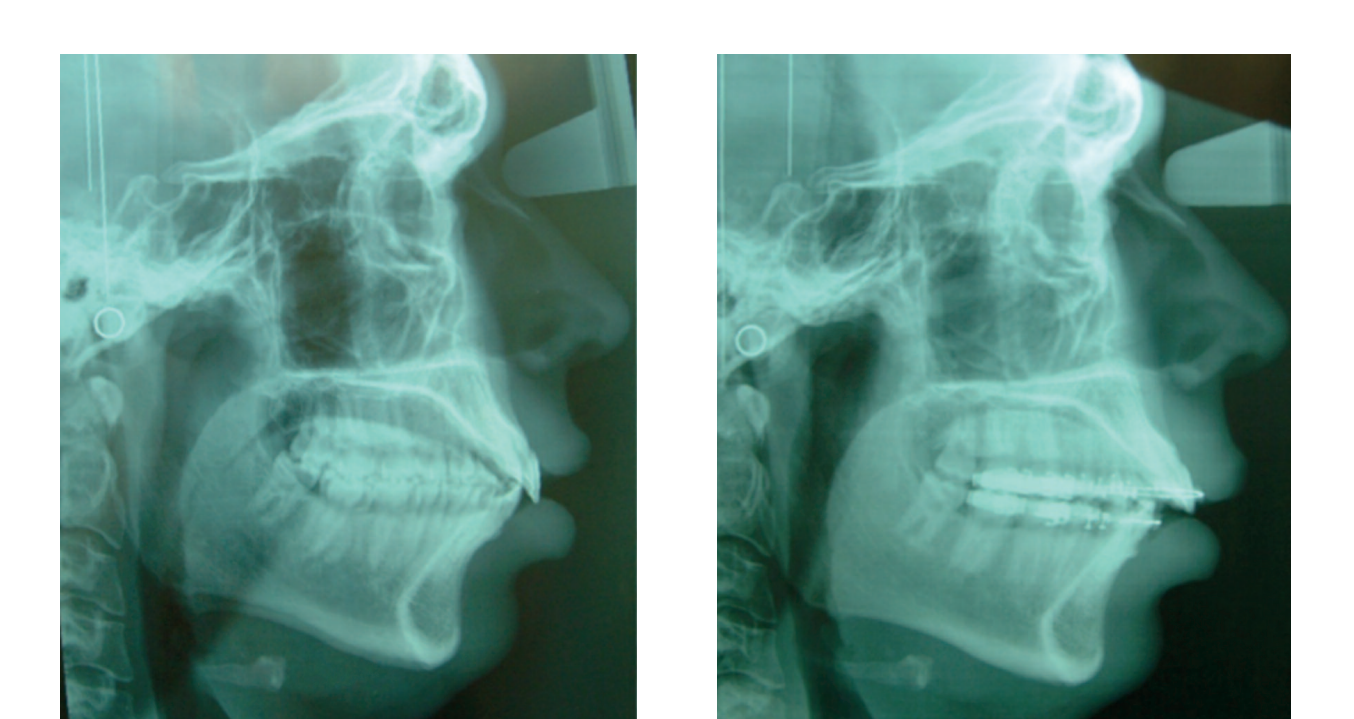
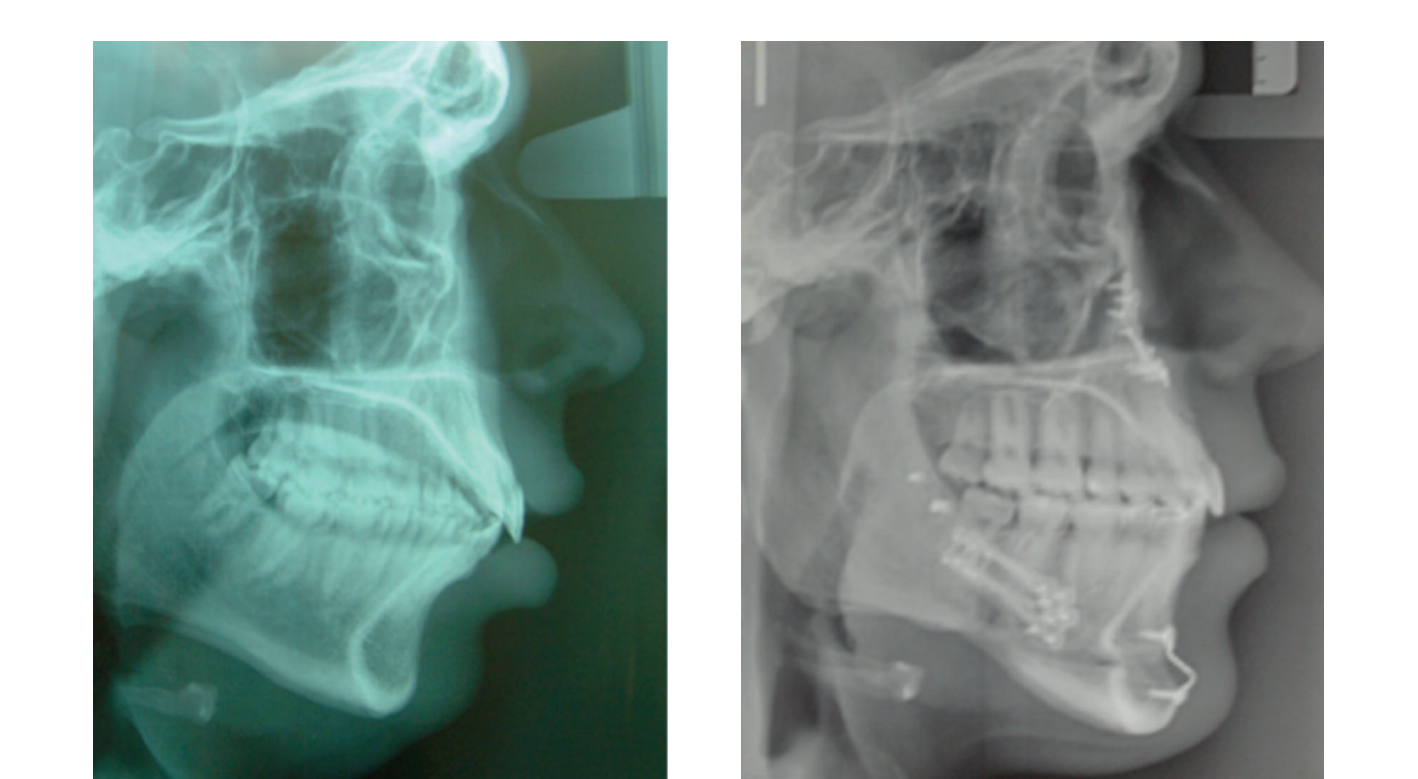
L'espansione scheletrica ha provocato un miglioramento delle vie aeree, come mostrano le sovrapposizioni radiologiche.
Conclusioni
Le deformità dentofacciali colpiscono il 10-15% della popolazione con vari gradi di coinvolgimento estetico o funzionale, che possono riguardare solo un mascellare o l'intero viso.
Questo caso rappresenta il paradigma dei nuovi cambiamenti nel modo di pensare alla chirurgia ortognatica. Non solo si ottiene uno stato occlusale soddisfacente, ma questa chirurgia ci offre l'opportunità di ottenere risultati estetici e funzionali migliori, che non sono comparabili con altri approcci chirurgici.
Individui con deformità moderata trasformano la loro estetica, e i miglioramenti vanno oltre, poiché non esiste altra tecnica comparabile alla chirurgia ortognatica che provochi cambiamenti nelle vie respiratorie come la chirurgia di avanzamento bimaxillare con cambiamento del piano occlusale. In questo paziente la chirurgia ha provocato un'espansione scheletrica.
Il miglioramento nell'aspetto ha una profonda importanza per come gli individui si giudicano e come la società li osserva. Ha un grande impatto sull'autostima. Il desiderio di migliorare l'aspetto è notevole nei pazienti con deformità, anche in quelli che dicono che le loro motivazioni sono funzionali, poiché è più facile giustificare così la necessità del trattamento.
La chirurgia ortognatica è raccomandata per il trattamento della maggior parte di questi casi, ottenendo un'occlusione funzionale combinata con un miglioramento nella masticazione, nella respirazione e nella fonazione.
Molti dei nostri pazienti si rivolgono a noi per un trattamento ortodontico, ma il dovere del professionista risiede non solo nel raggiungimento di un obiettivo occlusale stabile, ma anche nel miglioramento dell'estetica facciale, con tutte le sue conseguenze psico-emozionali positive.
César Colmenero Ruiz, Elena Bonilla Morente, Silvia Rosón Gómez, Carmen Torres de la Torre
Bibliografia
- Bell WH. Revascularizzazione e guarigione ossea dopo osteotomia mascellare: uno studio su scimmie rhesus adulte. Oral Surg. 1960; 27: 269-277.
- Brevi BC, Fuma L, Pau M, Sesena E. Rotazione antioraria del piano occlusale nel trattamento dell'OSAS. J. Oral. Maxillofac Surg. 2011; 69 : 917- 923.
- Bloomquist JE, Ahlborg G, Isaakson S. Un confronto della stabilità scheletrica dopo avanzamento mandibolare e utilizzo di due tecniche di fissazione interna rigida. J. Oral Maxillofac. Surg. 1997; 55: 568-576.
- Noguchi N, Tsuji M. Un sistema di simulazione ortognatica che integra dati su denti, mascella e faccia utilizzando la cefalometria 3D. Int. J. Oral Maxillofac. Surg. 2007; 36: 640-5.
- Poulto DR, Ware WH. Trattamento chirurgico-ortognatico della grave retrusione mandibolare. Am. J. Orthod. 1971; 58: 244-252.
- Sarver DM. L'arco del sorriso. L'importanza della posizione degli incisivi nel sorriso dinamico. Am. J. Orthod. Dentofacial Orthop. 2001; 120: 98-111.
- Swennen GRJ, Mollemans W , Schutyser F. Pianificazione del trattamento tridimensionale per la chirurgia ortognatica nell'era dell'imaging virtuale. J. Oral Maxillofac. Surg. 2007; 67: 2080-87.