Valutazione dell’effetto meccanico di strumenti singoli con movimento reciprocante (sistema WaveOne) in canali radicolari contaminati
Il trattamento endodontico ha subito tanti cambiamenti negli ultimi decenni, in particolar modo sugli aspetti tecnici della terapia; infatti, la tecnica di strumentazione è stata l’argomento più discusso a causa delle grandi innovazioni tecnologiche avvenute in questo ambito.
I sistemi rotanti sono stati sviluppati sfruttando un movimento meccanico di rotazione continua che presenta svariati vantaggi come un tempo di strumentazione ridotto rispetto agli strumenti manuali, un’alta percentuale di riduzione della flora batterica presente all’interno dei canali e una preparazione più centrata nel lume canalare. In ogni caso, la tecnica di strumentazione manuale è stata la più utilizzata per anni e rimane, a oggi, la metodica più insegnata nei percorsi universitari. Recentemente è stato sviluppato un nuovo sistema di strumentazione endodontico e proposto a livello mondiale, si tratta del sistema automatico WaveOne di Dentsply-Maillefer, uno strumento singolo con movimento reciprocante in grado di pulire e sagomare il canale radicolare. La cinematica dello strumento è molto semplice: si tratta di un ampio raggio di rotazione nella direzione di taglio e un piccolo raggio in senso opposto, che permettono allo strumento di procedere lungo il percorso canalare (Figura 1).
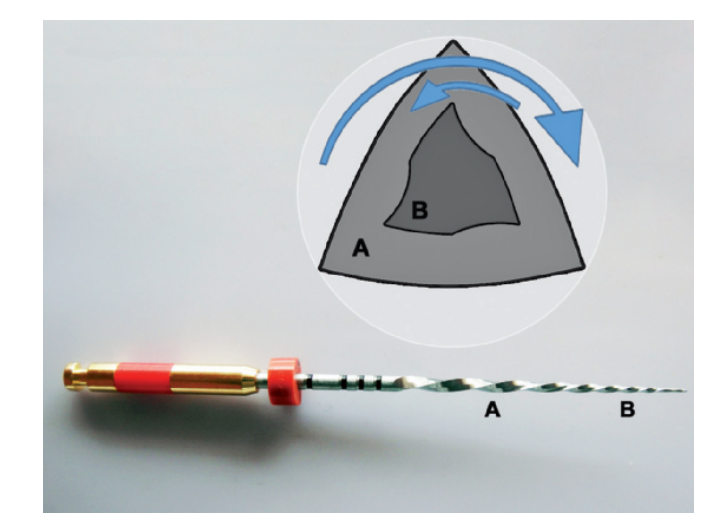
Questo movimento di reciprocazione diminuisce la fatica ciclica a cui è sottoposto lo strumento e, inoltre, i file sono realizzati con una lega speciale Ni-Ti, modificata con un procedimento termico, che viene denominata M-Wire e che ha proprietà di resistenza meccaniche superiori alle leghe Ni-Ti convenzionali.
Il sistema risulta anche più pratico e veloce di quelli tradizionali, riducendo di conseguenza la fatica nello svolgimento del lavoro e lo stress imposto al paziente. Tuttavia sono stati realizzati solo pochi studi sui sistemi con uno strumento unico reciprocante e mancano articoli che ne analizzino l’azione meccanica su canali contaminati. Lo scopo di questo studio è stato quindi di valutare la riduzione dei batteri presenti all’interno dei canali strumentati meccanicamente con sistema WaveOne, comparandoli con la strumentazione manuale.
Materiali e metodi
In questo studio sono stati analizzati 32 canali disto-vestibolari di molari superiori dritti, singoli, con una lunghezza standard di 12 mm. I canali sono stati strumentati a una lunghezza di lavoro di 11 mm, partendo con un K file #8 fino ad arrivare a un K file #15 (Dentsply Maillefer, Ballaigues, VD, Switzerland). L’apice è stato coperto con della resina e anche l’esterno della radice, apice incluso, è stato sigillato con resina epossidica (Araldite, Brascola, Joinvile, SC, Brazil).
I campioni sono stati quindi fissati su dei supporti in polistirene da 24 provette e bloccati con resina acrilica. Entrambi i supporti con i campioni installati sono stati sterilizzati con ossido di etilene (Acecil, Campinas, SP, Brazil).
È stata preparata una sospensione di Enterococcus faecalis (ATCC 29212) in un brodo di soia triptico (TSB, Difco, Le Pont de Claix, RA, France) e standardizzata al valore 4 della scala di McFarland e, sotto a una cappa ad aria filtrata, sono stati contaminati i canali con la sospensione di E. faecalis utilizzando una siringa da insulina. I supporti sono stati chiusi e incubati a 37° per 21 giorni e il contenuto dei canali è stato irrigato con TSB fresco ogni 48 ore.
Dopo il periodo d’incubazione, i canali sono stati riempiti con acqua sterile e i campioni di acqua contaminata sono stati raccolti con un cono di carta sterile #15 (Dentsply Maillefer, Ballaigues, VD, Switzerland) inserito per un minuto all’interno del canale. In seguito le punte sterili sono state conservate in provette contenenti 500 µL di TSB e sono state preparate delle diluizioni predeterminate per le analisi della presenza batterica.
I batteri sono stati quantificati in base al numero di colonie formate per mL (CFU/mL) dopo aver inserito le differenti diluizioni dei campioni prelevati nei supporti di coltura agar con m-Enterococcus (Difco, Le Pont de Claix, RA, France) e incubati a 37° per 48 ore.
I campioni sono stati quindi divisi in due gruppi (n=15) secondo le diverse tecniche di strumentazione:
Il Gruppo 1 è stato preparato con sistema WaveOne (Dentsply Maillefer, Ballaigues, VD, Switzerland) secondo le linee guida indicate dalla ditta produttrice.
È stato utilizzato il “primary file” (25.08) con il motore in sequenza reciprocante, facendolo penetrare prima nel terzo coronale ed estraendolo poi allo stesso modo nel terzo medio e in seguito terzo cervicale, fino a raggiungere la lunghezza di lavoro determinata. È stata effettuata dell’irrigazione con acqua distillata e un’esplorazione manuale con K file #15 dopo ogni passaggio di inserimento ed estrazione del file reciprocante. L’ultima irrigazione è stata realizzata con 5 ml di acqua distillata usando una siringa con punta da 29-gauge NaviTip (Ultradent Products, South Jordan, UT, USA).
Il Gruppo 2 è stato preparato con una tecnica di strumentazione manuale (Dentsply Maillefer, Ballaigues, Switzerland) secondo quanto descritto da Machado et al.14. I terzi cervicali e medi sono stati allargati con frese Gates-Glidden di misura da 1# a 3# (Dentsply Maillefer, Ballaigues, VD, Switzerland) e in seguito i canali sono stati preparati con una sequenza di diametro crescente di file fino a raggiungere la lunghezza di lavoro con K file #35. I canali radicolari sono stati quindi irrigati con acqua distillata che veniva applicata nuovamente dopo ogni singolo passaggio con strumenti manuali e, infine, irrigati con altri 5 mL di soluzione una vola terminata la preparazione, come nel Gruppo 1.
Il Gruppo di controllo era costituito da due campioni non contaminati, di cui uno è stato strumentato come nel Gruppo 1, mentre l’altro come nel Gruppo 2. Dopo l’irrigazione finale i canali sono stati di nuovo riempiti con acqua distillata e sono stati raccolti i campioni con le punte di carta sterile per quantificare la colonizzazione batterica residua come descritto precedentemente. La conta batterica è quindi stata verificata sia prima che dopo la strumentazione e la percentuale di riduzione è stata registrata. I dati raccolti sono stati processati statisticamente con l’U test di Mann-Whitney per poterne valutare il livello di significatività statistico (significatività al 5%, p<0,05).
Risultati
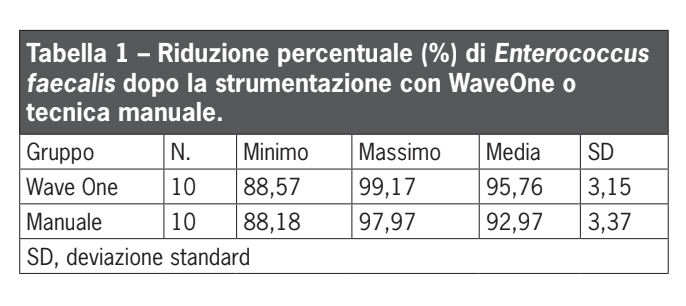
La valutazione della differenza tra i valori pre- e post-strumentazione ha evidenziato una riduzione media della carica batterica del 95,76% nel Gruppo WaveOne e del 92,97% nel Gruppo con tecnica manuale. Non sono state evidenziate differenze statisticamente significative tra i due gruppi (p>0,05). I dati statistici sono mostrati nella Tabella 1.
Non è stata evidenziata la presenza di popolazione batterica nel Gruppo controllo, confermando quindi le condizioni di sterilità nelle quali è stato effettuato l’esperimento.
Discussione
Una riduzione dei tempi di lavoro è sicuramente un grande vantaggio delle tecniche dell’Odontoiatria moderna, ma è di fondamentale importanza valutare se queste nuove tecniche portano a risultati migliori o simili a quelli delle tecniche convenzionali.
L’effetto dell’azione meccanica degli strumenti endodontici sulla rimozione dei batteri presenti va attentamente valutata. Alcuni ceppi batterici come Enterococcus faecalis possono infatti persistere nel sistema canalare per lunghi periodi, anche in zone povere di nutrienti per i batteri, portando al fallimento delle terapie endodontiche. La tecnica di contaminazione usata in questo studio, con 21 giorni di persistenza di Enterococcus faecalis, permette l’aumento della presenza batterica all’interno del canale e la sua organizzazione in bio-film.
Il trattamento endodontico è una procedura chimico-meccanica che consiste in una combinazione di azione di strumentazione dei canali e di utilizzo di prodotti chimici come irriganti, medicazioni antibatteriche e cementi.
Alla tecnica di strumentazione presentata in questo studio non è stato associato l’utilizzo di irriganti, poiché lo scopo era quello di comparare l’azione meccanica di rimozione di batteri di due tecniche di strumentazione diverse, senza l’interferenza dovuta all’effetto di soluzioni chimiche.
I risultati dello studio hanno sottolineato come la riduzione della popolazione batterica ottenuta con il sistema WaveOne fosse simile al gruppo strumentato manualmente, in accordo quindi con precedenti lavori che hanno mostrato similitudini tra tecniche manuali e di strumentazione meccanica automatizzata.
Entrambe le tecniche, WaveOne e strumentazione manuale, utilizzano la cinematica proposta da Roane et al., ovvero l’impiego di un ampio raggio di rotazione dello strumento in senso antiorario per tagliare la dentina e un piccolo arco in senso orario per procedere con il file all’interno del sistema canalare. La principale differenza tra i due sistemi è che la tecnica WaveOne si avvale di un sistema meccanico basato su un motore specifico che produce un movimento automatizzato reciprocante durante la sagomatura del canale.
Questo sistema è disponibile con tre file di dimensioni diverse: “small” (21.06), “primary” (25.08) e “large” (40.08); la scelta dipende dal diametro del canale. In questo studio è stato utilizzato il file “primary” perché la sonda di esplorazione utilizzata inizialmente era un K file #15.
Sono stati svolti molti studi sui premolari per valutare la riduzione dei batteri presenti, ma i molari fanno parte di quel gruppo di denti che più spesso è soggetto a terapie endodontiche; per questo motivo sono stati utilizzati nello studio, in modo da avvicinarsi il più possibile alla realtà clinica.
Inoltre i premolari hanno spesso un diametro più ampio di quello dei molari, per questo motivo in certi casi sarebbe stato più indicato il file WaveOne “large”. È stato scelto di utilizzare il file “primary” di WaveOne perché, in accordo con la casa produttrice, è quello utilizzato per la maggior parte dei canali radicolari.
I canali mesio-vestibolari e palatali dei molari sono stati invece esclusi poiché sarebbe stato difficile isolarli e decontaminarli correttamente, rischiando quindi di influenzare la conta batterica. Inoltre, la standardizzazione del canale mesio-vestibolare sarebbe risultata particolarmente complessa per la presenza del quarto canale.
La sagomatura dell’apice radicolare nel Gruppo con tecnica manuale è stata effettuata con un K file #35, mentre nel Gruppo WaveOne la punta dello strumento era di misura differente (#25). L’uso di diametri in punta differenti è giustificato dal fatto che con le tecniche di sagomatura con strumenti automatici, come ProTaper, è possibile procedere con la chiusura anche con coni master in guttaperca che abbiano un diametro apicale più largo dell’ultimo strumento usato perché la sagomatura dei rotanti è più ampia dell’ultimo file con movimento automatico utilizzato.
WaveOne presenta la stessa caratteristica; questa osservazione, infatti, sembra essere concorde con i risultati ottenuti in questo studio.
La differente sagomatura può anche essere motivata dalla diversa conicità, che per gli strumenti manuali è pari al 2% mentre è dell’8% nel caso dello strumento “primary” WaveOne.
Per quanto riguarda invece la sagomatura del terzo medio e terzo coronale del canale, nel caso della tecnica manuale sono state usate frese di Gates-Glidden, producendo quindi una svasatura maggiore, non influendo tuttavia sulle differenze tra i due gruppi in termini di riduzione di presenza batterica.
Nessun campione è invece risultato completamente privo di batteri, in contraddizione con quanto espresso da Coldero et al. che osservava come l’81% dei campioni strumentati con tecnica manuale avesse presenza batterica pari allo zero. Questa apparente contraddizione va valutata con attenzione: può essere, infatti, che le differenze osservate siano in realtà legate a limitazioni metodologiche; una piccola crescita batterica non può essere osservata con i metodi standard di coltura cellulare.
È interessante osservare come il sistema automatico WaveOne sia stato in grado di rimuovere il 95,76% dei batteri presenti senza l’utilizzo aggiuntivo di prodotti chimici, ottenendo un risultato paragonabile alle tecniche convenzionali ma in un tempo minore e senza perderne in qualità.
Conclusioni
L’azione meccanica del sistema WaveOne sui canali radicolari infetti produce una riduzione della carica batterica paragonabile a quanto ottenuto con la tecnica classica di strumentazione manuale.
Manoel Eduardo de Lima Machado, Cleber Keiti Nabeshima, Mário Francisco de Pasquali Leonardo, Felipe Britto de Lima Machado, Maria Leticia Borges Britto, Silvana Cai
Bibliografia
- Guelzow A, Stamm O, Martus P, Kielbassa AM. Comparative study of six rotary nickel- titanium systems and hand instrumentation for root canal preparation. Int Endod J 2005;38(10):743-52.
- Peru M, Peru C, Mannocci F, Sheriff M, Buchanan LS, Pitt Ford TR. Hand and nickel-titanium root canal instrumentation performed by dental students: a micro-computed tomography study. Eur J Dent Educ 2006;10(1):52-9.
- Yin X, Cheung GS, Zhang C, Masuda YM, Kimura Y, Matsumoto K. Micro-computed tomographic comparison of nickel-titanium rotary versus traditional instruments in C-shaped root canal system. J Endod 2010;36(4):708-12.
- Chuste-Guillot M-P, Badet C, Peli J-F, Perez F. Effect of three nickel-titanium rotary file techniques on infected root dentin reduction. Oral Surg Oral Med Oral Pathol Oral Radiol Endod 2006;102(2):254-8.
- Machado MEL, Sapia LAB, Cai S, Martins GHR, Nabeshima CK. Comparison of two rotary systems in root canal preparation regarding disinfection. J Endod 2010;36(7):1238-40.
- Taşdemir T, Aydemir H, Inan U, Ünal O. Canal preparation with Hero 642 rotary Ni- Ti instruments compared with stainless steel hand K-file assessed using computed tomography. Int Endod J 2005;38(6):402-8.
- Aguiar CM, Mendes DA, Câmara AC, Figueiredo JAP. Evaluation of the centreing ability of the ProTaper Universal rotary system in curved roots in comparison to Nitiflex files. Aust Endod J 2009;35(3):174-9.
- De-Deus G, Moreira EJL, Lopes HP, Elias CN. Extended cyclic fatigue life of F2 ProTaper instruments used in reciprocating movement. Int Endod J 2010;43(12):1063-8.
- You S-Y, Kim H-C, Bae K-S, Baek A-H, Kum K-Y, Lee WC. Shaping ability of reciprocating motion in curved root canals: a comparative study with micro-computed tomography. J Endod 2011;37(9):1296-300.
- Plotino G, Grande NM, Testarelli L, Gambarini G. Cyclic fatigue of Reciproc and WaveOne reciprocating instruments. Int Endod J 2012;45(7):614-8.
- Pereira ES, Peixoto IF, Viana AC, Oliveira II, Gonzalez BM, Buono VT et al. Physical and mechanical properties of a thermomechanically treated NiTi wire used in the manufacture of rotary endodontic instruments. Int Endod J 2012; 45(5): 469-474.
- Ye J, Gao Y. Metallurgical characterization of M-Wire nickel-titanium shape memory alloy used for endodontic rotary instruments during low-cycle fatigue. J Endod 2012;38(1):105-7.
- Bürklein S, Hinschitza K, Dammaschke T, Schäfer E. Shaping ability and cleaning effectiveness of two single-file systems in severely curved root canals of extracted teeth: Reciproc and WaveOne versus Mtwo and ProTaper. Int Endod J 2012;45(5):449-61.
- Machado MEL, Shin RCF, Zólio AA, Pallotta RC, Nabeshima CK. Confronto tra la quantità di sigillante nell’otturazione canalare con l’uso di strumentazione e tecniche d’otturazione diverse. Il Dent Mod 2010;28:50-6.
- Sedgley CM, Lennan SL, Appelbe OK. Survival of Enterococcus faecalis in root canals ex vivo. Int Endod J 2005;38:735-42.
- Berber VB, Gomes BPFA, Sena NT, Vianna ME, Ferraz CCR, Zaia AA, Souza-Filho FJ. Efficacy of various concentrations of NaOCl and instrumentation techniques in reducing Enterococcus faecalis within root canal and dentinal tubules. Int Endod J 2006;39:10-7.
- Dalton BC, Ørstavik D, Pettiette M, Trope M. Bacterial reduction with nickel-titanium rotary instrumentation. J Endod 1998;24(11):763-7.
- Siqueira Jr JF, Lima KC, Magalhães FAC, Lopes HP, Uzeda M. Mechanical reduction of the bacterial population in the root canal by three instrumentation techniques. J Endod 1999;25(5):332-5.
- Matos Neto M, Santos SSF, Leão MVP, Habitante SM, Rodrigues JRDD, Jorge AOC. Effectiveness of three instrumentation systems to remove Enterococcus faecalis from root canals. Int Endod J 2012;45:435-438.
- Roane JB, Sabala CL, Duncanson Jr MG. The ‘balanced force’ concept for instrumentation of curved canals. J Endod 1985;11(5):203-11.
- Singla M, Aggarwal V, Logani A, Shah N. Comparative evaluation of rotary ProTaper, Profile, and conventional stepback technique on reduction in Enterococcus faecalis colony-forming units and vertical root fracture resistance of root canals. Oral Surg Oral Med Oral Radiol Oral Pathol Endod 2010;109:e105-10.
- Gorduysus M, Nagas E, Torun OY, Gorduysus O. A comparison of three rotary systems and hand instrumentation technique for the elimination of Enterococcus faecalis from the root canal. Aust Endod J 2011;37:128-33.
- Araquam KR, Britto MLB, Nabeshima CK. Comparison of two single-cone obturation techniques. ENDO (Lond Engl) 2011;5(2):133-7.
- Coldero LG, McHugh S, Mackenzie D, Saunders WP. Reduction in intracanal bacteria during root canal preparation with and without apical enlargement. Int Endod J 2002;35(5):437- 46.
- Siqueira Jr JF, Rôças IN. Exploiting molecular methods to explore endodontic infections. Part 1: Current molecular technologies for microbiological diagnosis. J Endod 2005;31(6):411-23.