
Orthodontics and Orthognathic Surgery in Class II Dolichofacial Patients: Occlusal Plane Change
Traduzione automatica
L'articolo originale è scritto in lingua EN (link per leggerlo) .
For a time, counterclockwise mandibular rotation through osteotomies was considered an unpredictable procedure with a high rate of relapse and postoperative open bites.
Changes in the design of osteotomies and the emergence of rigid osteosynthesis allow for counterclockwise rotation of the occlusal plane, resulting in a significant optimization of aesthetics and function.
We present a case of orthodontic treatment and orthognathic surgery in a patient with significant joint symptoms, class II, and severe dolichofacial pattern treated with bimaxillary surgery with occlusal plane change.
Caso Clínico
The 21-year-old patient came to consultation presenting orthodontic treatment performed in another clinic and was not satisfied with the evolution.
Diagnóstico:
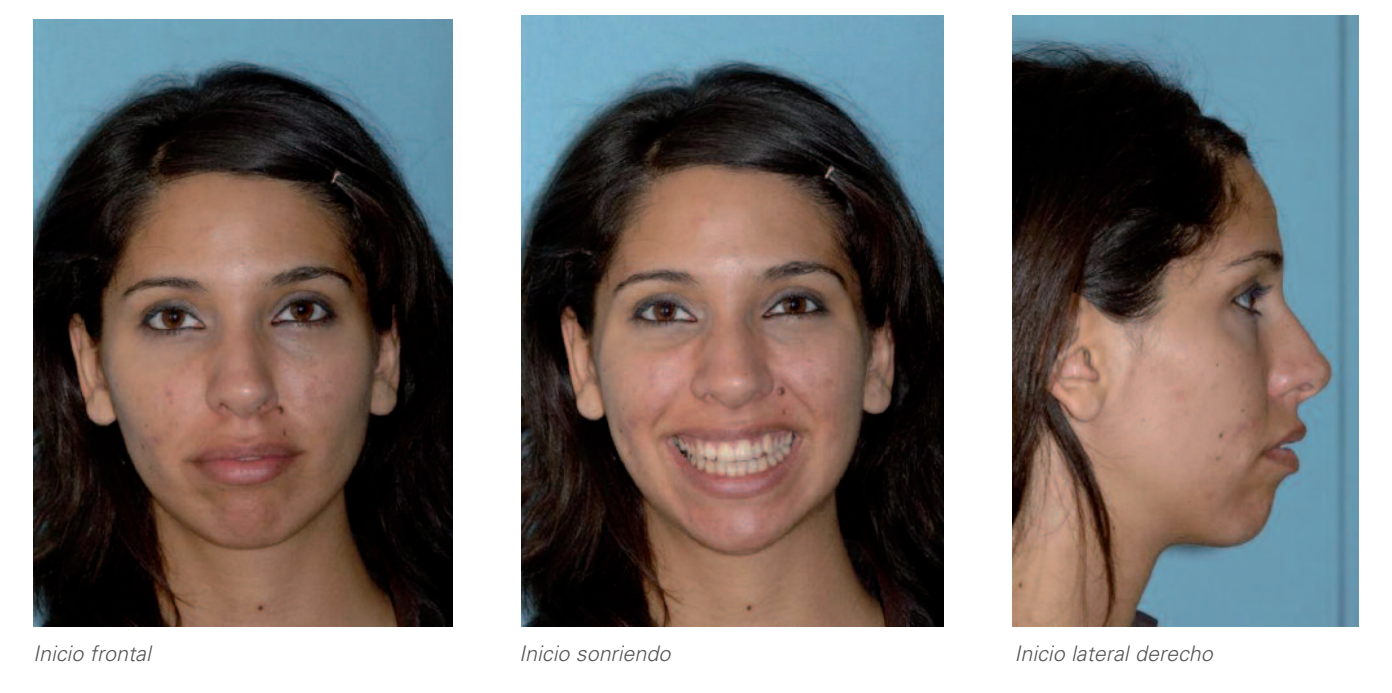
1. Análisis extraoral:
Incompetencia labial.
Contracción de la musculatura perioral en sellado.
Eversión del labio inferior.
Adecuada exposición de incisivos en sonrisa.
Estética de la sonrisa alterada por la marcada torsión positiva de los caninos superiores (especialmente el izquierdo) y la ligera torsión negativa de los premolares, que en conjunto proporcionan una sensación de arcada superior estrecha.
Perfil convexo.
Mentón retrognático.
Proquelia superior.
Marcado ángulo mentolabial.
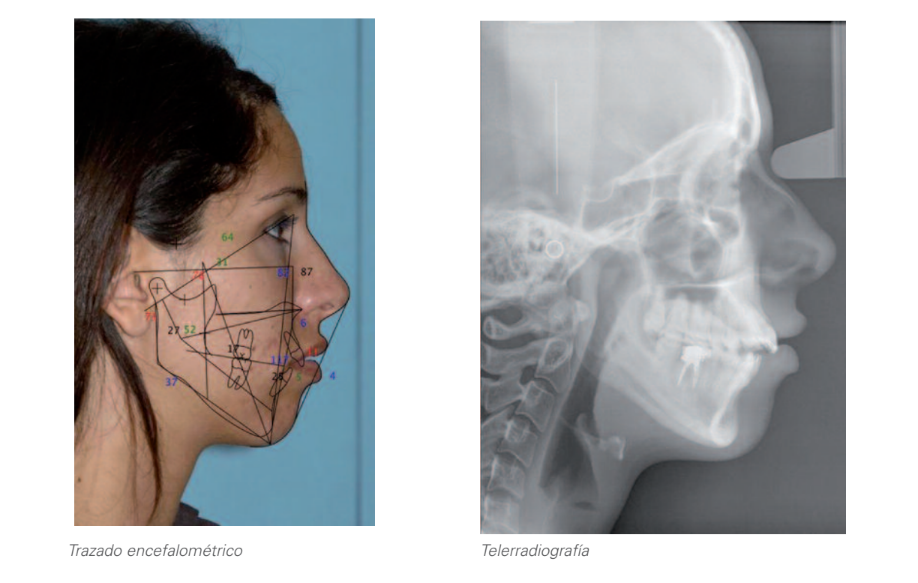
2. Análisis radiográfico:
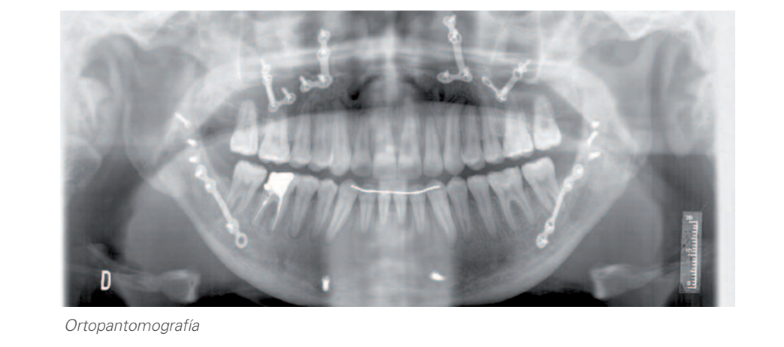
2.1. Ortopantomografía:
Dentición permanente.
Alteración morfológica en ambos cóndilos, siendo además el izquierdo marcadamente menor en tamaño.
Imagen radiolúcida en ambas raíces y la zona de la furca del 46.
Ausencia de: 38, 48.
2.2. Teleradiografía lateral de cráneo y trazado cefalométrico:
Dolicofacial severo.
Clase II ósea causa mandibular.
Biprotrusión dentaria.
3. Análisis intraoral:
Mordida abierta: 0,5mm.
Resalte: 6mm.
Lado derecho: Clase II molar y canina.
Lado izquierdo: Clase I molar y clase II canina.
Desviación de línea media inferior 0,5mm hacia la derecha.
Discrepancia óseo-dentaria inferior: -2,5mm.
Desgastes dentarios en los sectores posteriores.
Biotipo periodontal fino.
Recesión gingival en el 34.
4. Analysis of mounted models in articulator:
Prematurity in 28-37.
Severe worsening of the vertical and sagittal problem.
Treatment plan
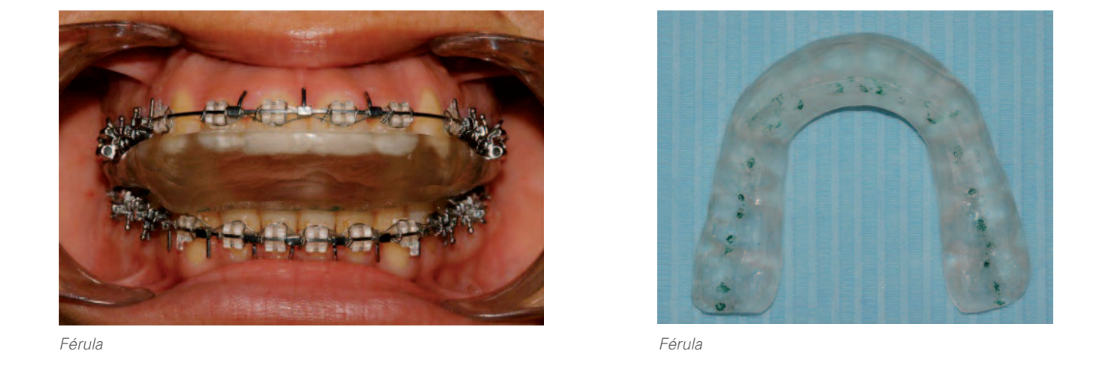
When presenting the patient with a morphological alteration of both condyles, the smaller size of the left condyle compared to the right and the marked difference between maximum intercuspation and centric relation, it was decided to start by placing a splint in order to obtain a stable condylar position and highlight the true magnitude of the vertical and sagittal problem, in order to be able to make a diagnosis of the patient's three-dimensional problem having ruled out joint compensation. The patient was warned that the condylar position obtained after its use is not always reversible and that it would almost certainly lead to a combined treatment of orthodontics and orthognathic surgery.
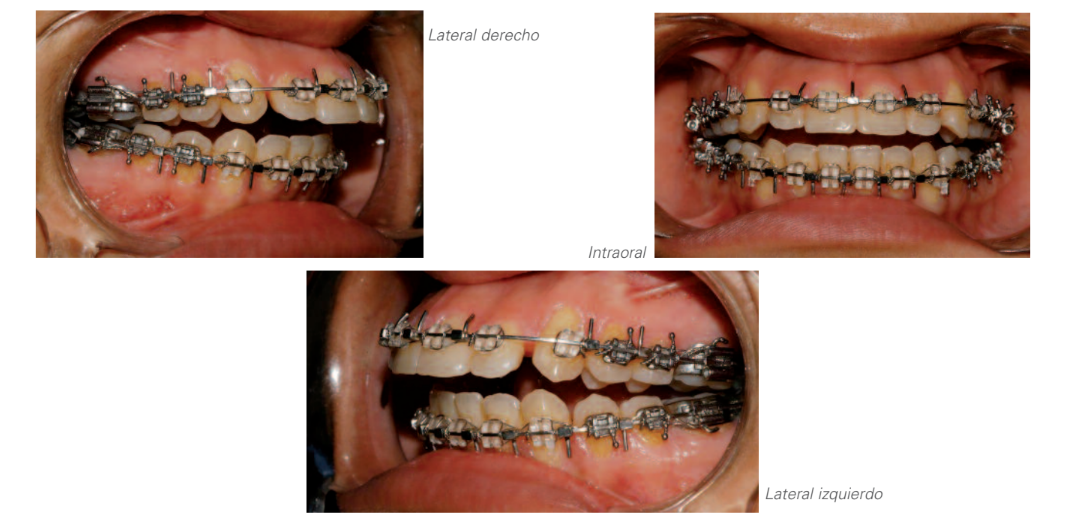
After the use of the splint, posterior mandibular rotation was observed with the consequent increase in lower vertical dimension, overjet, class II, and open bite; as well as greater labial incompetence and mandibular retrusion.
As is routinely done in any case when planning a treatment plan, treatment objectives were established for the different areas that would be affected by it, serving as a framework for communication with the patient and among different professionals, as well as a critical element for the evaluation of the results obtained. These objectives were:
Facial aesthetics.
Dental aesthetics.
Functional occlusion.
Periodontal health.
Stability.
Patient satisfaction.
En base a ello y buscando quedar lo más cerca posible del grado máximo de cumplimiento en cada una de las citadas áreas, se le presentó a la paciente una única opción de tratamiento (ortodoncia combinada con cirugía ortognática) debido a su estado articular, a la magnitud de los movimientos dentarios que sería necesario realizar para cumplir los objetivos a nivel de oclusión funcional y al posible empeoramiento de la condición periodontal al forzar los dientes respecto al hueso alveolar, en caso de haber intentado una compensación dentoalveolar al problema óseo, y la plausible mejoría en la estética facial.
Estudio inicial


Oclusión después de la férula

Combined orthodontic treatment with orthognathic surgery:
Orthodontics:
During the treatment planning phase, it was decided that the patient's temporomandibular joints constituted an important limiting factor when considering the pre-surgical orthodontics to be performed, estimating that a shorter treatment time associated with less dental displacement could represent a potential decrease in the risk of condylar resorption. Thus, the multidisciplinary team assumed the inherent limitation of an incomplete compensation of dental protrusion.
Once the pre-surgical orthodontics was completed, the joint position was stabilized again, also seeking to avoid errors in the final surgical planning.
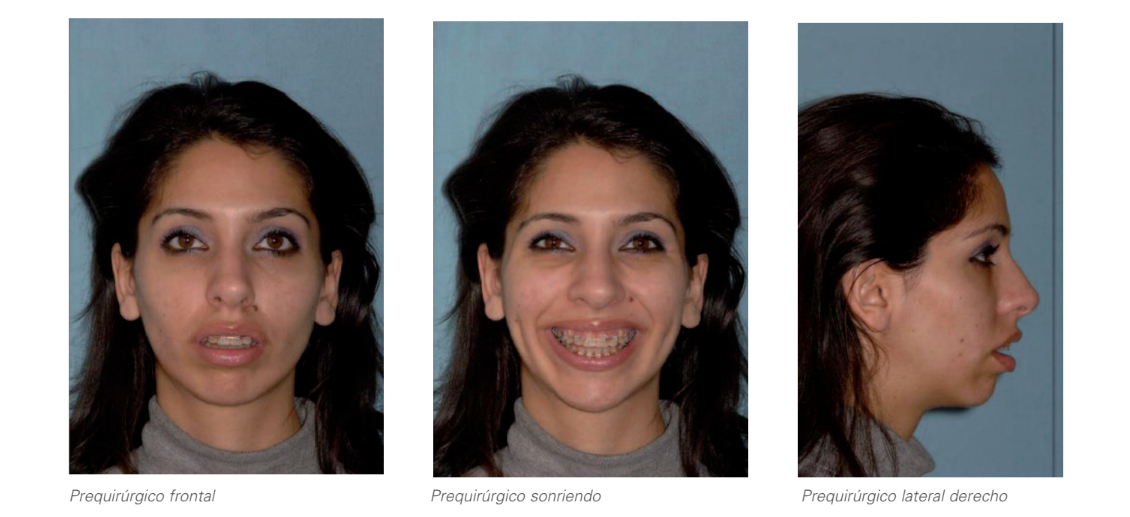
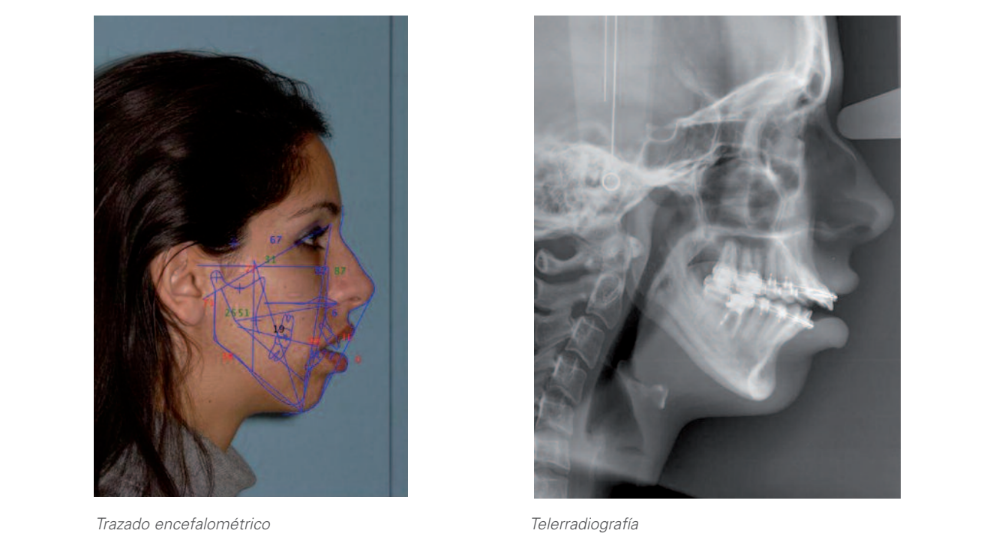
Preoperative study


Oclusión prequirúrgica post férula
Surgery:
Under general anesthesia, a multisegmental Lefort-1 osteotomy was performed between the lateral incisors and canines; maxillary expansion of 6 mm was performed at the molar level and 3 mm at the canine level. The segmentation allowed for control of the torque of the anterior segment, impacting 4 mm in its anterior portion, advancing the maxilla by 3 mm. The nasal septum was trimmed by 5 mm to avoid interferences. These movements generated a significant open bite that was closed through mandibular sagittal osteotomy, performing a significant detachment of the distal fragment and rigid fixation with miniplates and bicortical position screws. Once the occlusion was verified, two class II elastics were placed. The anterior fragment of the maxilla was left unfixed, and a skeletal traction wire was placed in the anterior nasal spine. The muscles of the upper lip and perinasal structures were reconstructed, performing a v-y closure and alar sling.
Finally, the surgery ended with a genioplasty of advancement of 5 mm and vertical reduction of 3 mm.
The patient was extubated in the operating room and discharged 24 hours later with two soft class II elastics and another skeletal from the maxillary incisal fragment to the chin.
Post-surgical orthodontics:
In the post-surgical orthodontics stage, the occlusion was finalized.
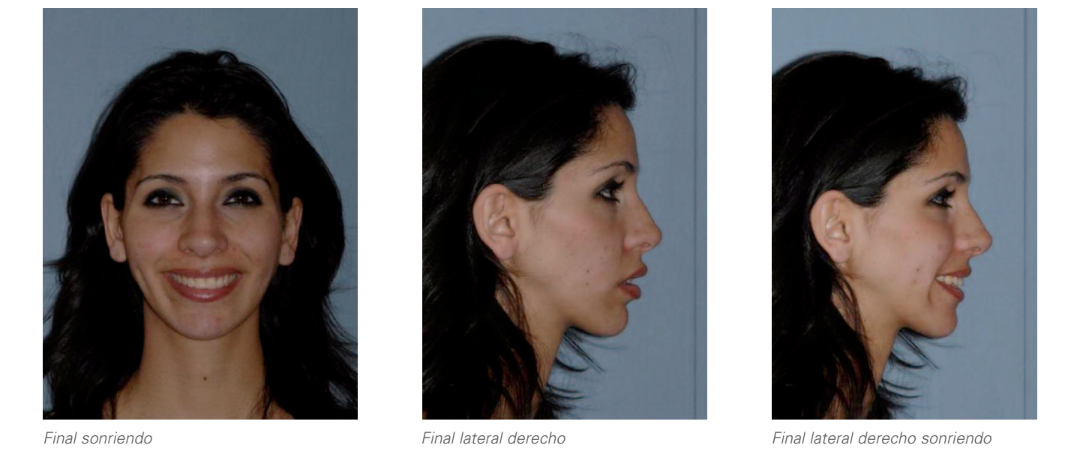
Final study


El presente caso pone de manifiesto la importancia en ortodoncia del diagnóstico de la existencia de compensación articular e intensidad de la misma, dada la eventual fuente de errores que podrían surgir de no ser tenida en cuenta en el diagnóstico, planificación y ejecución del tratamiento al alterar las relaciones espaciales entre las bases óseas mandibular y maxilar con sus respectivas arcadas y afectar por ello al plan de tratamiento de las distintas alternativas planteables. A su vez, se destaca la importancia de un adecuado y cuidadoso manejo ortodóncico-quirúrgico de los problemas esqueléticos derivados de una importante reabsorción condilar, para la obtención de una adecuada estética facial y dental, una correcta oclusión funcional, manteniendo la salud periodontal.
Retención



Conclusiones
El tratamiento de las compensaciones articulares previo al tratamiento de ortodoncia y cirugía permite desenmascarar la deformidad oclusal y facial en su totalidad y realizar así una correcta planificación. La cirugía bimaxilar con cambio de plano oclusal en pacientes dolicofaciales supone una mejora estética considerable y una mejoría en el patrón respiratorio en este subgrupo de pacientes tan complicado.
Comparativa prequirúrgico - situación final

Fe Serrano Madrigal, César Colmenero Ruíz, Javier Prieto Serrano, Teresa Martínez Iturriaga
Bibliografía
- Ellis E, Gallo WJ. Un método para predecir con precisión la posición del incisivo maxilar en cirugía bimaxilar. J.O.M.S. 42: 402-410. 1984.
- Wolford LM, Chemello PD, Hilliard FW. Alteración del plano oclusal en cirugía ortognática. J.O.M.S. 51: 730-744. 1993.
- Stansbury C, Evans C, Miloro M. Estabilidad de la corrección de mordida abierta con osteotomía de división sagital y rotación de cierre de la mandíbula. J.O.M.S. 68: 149-159. 2010.
- Ow A, Kwong LC. Estabilidad esquelética y complicaciones de la osteogénesis por distracción mandibular y división sagital bilateral. Una revisión basada en evidencia. J.O.M.S. 67: 2344-2353. 2009.